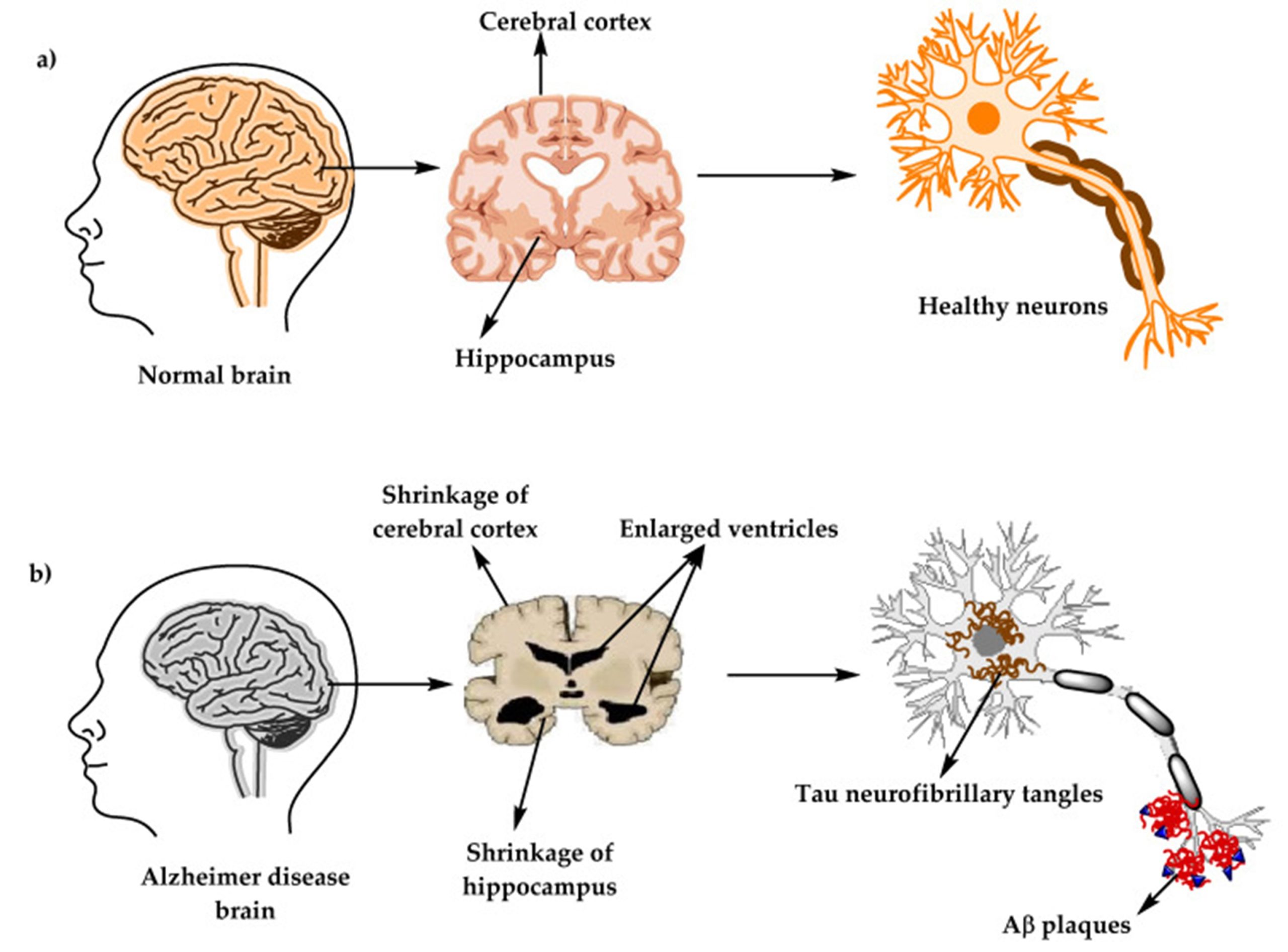
(Image: Structure of a healthy brain versus a brain observed in Alzheimer’s disease, adapted from Brejyeh and Karaman, 2020)
Normally, these proteins are disposed of as waste, but this process requires the proper involvement of three enzymes (α-, β- and γ-secretase) that cut the proteins. When either of these enzymes show abnormal activity, the beta-amyloid proteins accumulate around the outside of neurons, forming plaques that interfere with communication between neurons. This eventually leads to the cell death of neurons and shrinkage of cortex (brain tissue), in areas needed for language, memory and planning.
Another common explanation is the formation of tangles within the neuron cells composed of tau protein. These tangles are known as neurofibrillary tangles, and although both are considered biomarkers that indicate whether a person has Alzheimer’s disease, scattered amyloid protein plaques can be found commonly in brains of older persons who do not have Alzheimer’s disease. Neuritic plaques where the amyloid protein is more densely packed among neurites that have been distorted by neurofibrillary tangles are considered to be a more specific marker for Alzheimer’s disease.